To his great credit, Bowles reiterated yesterday that a core principle of deficit reduction must be to “protect the disadvantaged.” Unfortunately, his “compromise” between a serious Democratic offer and a Republican stand-pat offer would lead almost inevitably to a significant violation of this important principle.
We don't agree -- it is possible to achieve well over $600 billion in Medicare savings while actually helping the most vulnerable. Here is one possible formulation of how:
| Policy | Savings | Effect on the Disadvantaged | ||
| Helps | Little Effect | Hurts | ||
| Reduce Provider Payments | $175 billion | X | ||
| Prescription Drug Rebates | $112 billion | X | ||
| Restrict Medigap | $93 billion | X | ||
| Reform Cost Sharing | X | |||
| Raise the Eligibility Age | $125 billion | X | ||
| Medical Malpractice Reform | $62 billion | X | ||
| Increase Income-Related Premiums | $40 billion | X | ||
| Total Savings | $607 billion | $280 billion | $327 billion | $0 |
...According to a previous CBO analysis, the most vulnerable would actually be helped.
True, in a given year, most people (78 percent in their analysis) would experience higher cost sharing -- about $500 worth. But those with serious health expenses -- the top 9 percent in terms of health spending -- would see huge reductions in their out of pocket costs -- by about $4,500. If you do that math on that, it means that this option to reform cost-sharing would actually reduce mean cost sharing by $15 per person, due to the new protections being offered for those with high costs (which, though only a tenth of the population in a given year, will include the majority of beneficiaries at some point in their lifetime).
In other words, while beneficiaries cost-sharing expenses may be higher in any given year when they don't have major illnesses or medical conditions, beneficiaries would be protected from catastrophic health care costs, which are one of the leading causes of bankruptcy in the country. Now that's protecting the most vulnerable!
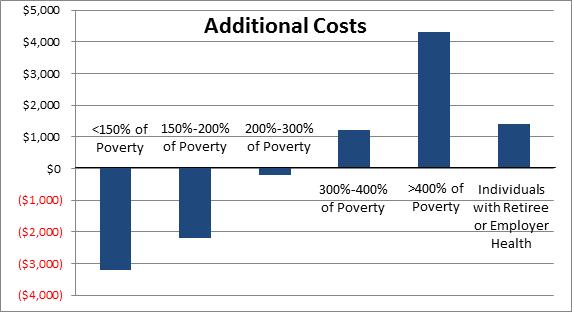
So who is it that sees their costs go down? You guessed it -- the most vulnerable and disadvantaged. Those with no employer coverage making less than 150 percent of the poverty line see on average a $3,000 reduction in costs, those under 200 percent a $2,000 reduction, and even those under 300 percent of poverty ($33,000 for an individual) see a reduction in their out-of-pocket costs.
...Adding it all up gets you to over $600 billion in savings without putting any additional burden on the most vulnerable Americans, and in many cases reducing their burden. And, of course, there are many other options out there to reform Medicare, Medicaid, TRICARE, FEHB, and other health programs, and to do so without imposing large new costs on those who rely most on those program.
The worst thing we could do for the most disadvantaged, though, is nothing. In a fiscal crisis scenario, we would be forced to make immediate cuts to spending and/or tax increases to bring the budget under control. It would be much more difficult under that scenario to protect the most vulnerable from budget reforms.